


By 2050, Pakistan’s population is projected by the WHO to rise by almost 50 percent, reaching 372 million. A growing population inevitably brings an increase in health-related challenges and expenditures.
While life expectancy in Pakistan remains below the global average (66 years compared with 71.4 years worldwide), the country is also grappling with one of the most serious health threats of our time: diabetes.
According to the International Diabetes Federation (IDF), Pakistan had 34.5 million adults aged 20–79 living with diabetes in 2024, ranking fourth globally behind China (148 million), India (90 million), and the United States (38.5 million). Projections suggest that by 2050, this number will rise to 70.2 million, moving Pakistan to third place globally.
What makes the situation particularly alarming is that Pakistan’s age-standardised diabetes prevalence is the highest in the world, at 31.4 percent in 2024. This means that nearly one in three adults in Pakistan is living with diabetes.
Among older adults, 4.2 million people aged 65–99 are already managing the condition, placing a growing burden on families caring for elderly relatives.
But what has brought Pakistan to these catastrophic levels?
Diet fuels the diabetes crisis:
The age-standardized diabetes rate in Pakistan is nearly 3.3 times that of India (10.5 percent) and 2.6 times that of Bangladesh (13.2 percent), two South Asian countries with broadly similar genetic backgrounds. This difference is driven not only by genetics and sedentary lifestyles but also by poor dietary habits. Pakistan’s consumption patterns are highly diabetogenic, accelerating the rise of diabetes across the population.
Per capita sugar consumption in Pakistan stands at approximately 33 kilograms annually, nearly double that of India, which also produces 17 percent of global sugar, and more than five times that of Bangladesh and China, where it is just over 6 kilograms (World Population Review).
The country’s oil-based diet further compounds the risk. Local consumption of edible oils is around 5 million metric tons, translating to roughly 22 kilograms per person. To meet this growing demand, Pakistan imports nearly 3 billion dollars’ worth of palm oil annually, reflecting rapidly accelerating local consumption.
===========================================================
Annual per capita consumption patterns - Pakistan vs Region
===========================================================
Sugar Edible oil Tea
Consumption consumption consumption
-----------------------------------------------------------
Pakistan 31.7 Kg 22 kg 1.5 kg
India 17.1 Kg 24 kg 0 3 kg
Bangladesh 6 09 Kg 9.4 kg 0.55 kg
===========================================================
Tea is another major contributor. Pakistan is the world’s top tea importer, with per capita consumption at 1.5 kilograms annually, compared with 0.3 kilograms in India and 0.55 kilograms in Bangladesh. With dietary patterns high in sugar, oil, tea, and refined carbohydrates, it is extremely difficult to curb the growing diabetes epidemic, which results in many preventable deaths.
It’s a deadly disease with minimum government spending:
Last year, diabetes-related deaths in Pakistan reached 0.23 million. To put this into perspective, China reported 0.76 million deaths, the United States 0.36 million, India 0.33 million, Indonesia 0.13 million, and Mexico 0.12 million.
The impact of diabetes extends beyond mortality. Each day, an estimated 35 to 40 Pakistanis undergo lower-limb amputations due to uncontrolled diabetes. If current trends continue, nearly 600,000 people could lose their legs every year. Most of these cases are preventable, but the lack of timely diagnosisand health expenditure has worsened the crisis.
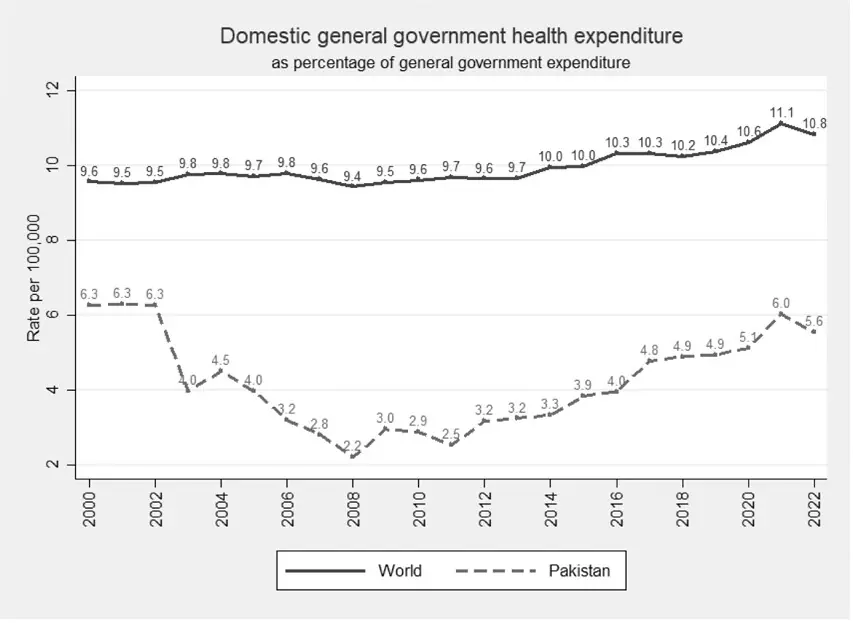
Pakistan spends far less on health than most countries with high diabetes prevalence, and this spending is declining. WHO data shows that the share of domestic government health expenditure fell from 6.3 percent in 2000 to just 5.6 percent in 2022, compared to the global average of 10.8 percent. Public funding for diabetes care is particularly limited.
The government spends only about USD 79 per person annually on diabetes prevention and treatment, among the lowest in the world and only slightly higher than countries with much lower prevalence such as Bangladesh (USD 74 per person for 13.8 million people) and the Democratic Republic of the Congo (USD 81 per person for 2.9 million people with diabetes).
This limited health spending contributes to diabetes-related deaths, but the larger crisis lies with the millions living with the disease, whose treatment costs and lost productivity are quietly straining Pakistan’s economy.
Lost human productivity:
International evidence shows how diabetes reduces workforce efficiency and labour market participation through increased absenteeism, unemployment, and early retirement.
In Australia, for example, diabetes reduced total years of life lived by nearly 3 percent and productivity-adjusted life years (PALYs) by 11.6 percent for men and 10.5 percent for women. The effect was most pronounced among young adults aged 20–24, where PALYs fell by 12.2 percent for men and 11 percent for women.
Similarly, in Germany, labour force participation among individuals without diabetes was 82.2 percent, compared to 55.9 percent among those with diabetes (Mackowiak et al., 2025). A study across 16 European countries also found that diabetes raises the likelihood of exiting the labor force by 30 percent (Rumball-Smith et al., 2014).
In Pakistan, where diabetes prevalence is high and health spending is low, the disease is causing major productivity losses, particularly among the working-age population. A recent study found that 76 percent of patients reported productivity losses, with work output dropping by 25 percent (Zafar et al., 2025).
These reductions in productivity and labour participation directly translate into economic losses for the country.
Economic cost of diabetes:
Pakistan lacks a dedicated healthcare budget for diabetes, forcing patients to bear treatment costs largely out of pocket. Mahmood and Adnan (2025) estimate the average monthly cost of diabetes management at PKR 5,591 (or PKR 67,092 annually), consuming nearly 19 percent of an average household’s income and ranging between 9 and 33 percent depending on individual circumstances.
Treatment costs also vary across cities. Total annual costs, including indirect expenses, were estimated at PKR 156,890 in Islamabad and PKR 134,220 in Karachi, with medications accounting for 43.2 percent of direct costs, followed by monitoring and consultations at 28.7 percent (Kumari et al., 2025).
For low-income households, insulin expenses alone can consume up to 30 percent of monthly income, and access remains a major barrier. Only about half of public health facilities maintain a regular insulin supply, worsening access and affordability (Bibi, Jiwani, and Das, 2024).
Beyond healthcare spending, productivity losses add heavily to the economic burden. Arshad, Alqahtani, and Rasool (2024) estimate productivity losses of USD 3.5 per diabetic patient annually (likely an underestimation). When extrapolated to Pakistan’s diabetic population of 34.5 million, this amounts to approximately USD 120.75 million (PKR 38 billion) in annual productivity losses to the nation.
Overall, the total economic cost of diabetes is projected to rise from PKR 320.21 billion in 2021 to PKR 411.17 billion by 2030, growing at 2.78 percent annually (Mahmood & Adnan, 2025).
The missing framework for diabetes care:
Despite the scale of the problem, Pakistan still lacks a coherent national strategy for diabetes prevention and control. The Diabetes Association of Pakistan introduced a National Action Plan for Diabetes, last updated in 2018, but implementation remains limited. The absence of a centralized diabetes registry and weak integration of screening into primary healthcare delay diagnosis and worsen management outcomes.
Genetics cannot be changed, but unless dietary habits improve and significant investment is made in healthcare, diabetes prevalence will continue to rise.
Public healthcare facilities are under-resourced, and private care is unaffordable for most, reinforcing inequities. Poorer households often forgo treatment to prioritize food and shelter, while rural and underserved urban areas have limited access to screening and care. As a result, many remain undiagnosed or unable to manage their condition. According to a WHO study, it takes an average of 4.5 days in Pakistan to access insulin, highlighting the fragility of the healthcare system and the growing diabetes crisis.
A healthy workforce is a nation’s most valuable asset. In Pakistan, rising diabetes is eroding that strength through lost productivity, higher economic costs, and preventable deaths. The failure to control this growing health crisis in one of the world’s most populous countries sends an urgent warning for the generations to come.
Copyright Business Recorder, 2025

PUBLIC SECTOR EXPERIENCE: He has served as Member Energy of the Planning Commission of Pakistan & has also been an advisor at: Ministry of Finance Ministry of Petroleum Ministry of Water & Power
PRIVATE SECTOR EXPERIENCE: He has held senior management positions with various energy sector entities and has worked with the World Bank, USAID and DFID since 1988. Mr. Shahid Sattar joined All Pakistan Textile Mills Association in 2017 and holds the office of Executive Director and Secretary General of APTMA.
He has many international publications and has been regularly writing articles in Pakistani newspapers on the industry and economic issues which can be viewed in Articles & Blogs Section of this website.
Sarah Javaid is an Economist by education and practice, with experience in the Ministry of Commerce, the textile sector, and think tanks. She has participated in the monitoring mission of the Pakistan Regional Economic Integration Activity for USAID. Her writings focus on international trade and export competitiveness. Currently, she serves as a Trade Economist at the All Pakistan Textile Mills Association


















Comments
Comments are closed for this article.